

What Is The Latest Version Of The Final Rule For The Ltch Pps In The Fedral Register?
Medicare & Medicaid Services (CMS) Aug. 2 issued its hospital inpatient prospective payment system (PPS) and long-term intendance infirmary (LTCH) PPS final rule for financial year (FY) 2022. In add-on to finalizing a two.five% increment in inpatient PPS payments for 2022 and other policies, the rule repeals the requirement to report sure payer-negotiated rates and makes changes to quality measurement and value programs. Highlights of the proposals related to the LTCH PPS are covered in a separate Special Bulletin. The regulations take outcome October. 1.
AHA Take
We appreciate CMS listening to our concerns by repealing the requirement that hospitals and health systems disembalm privately negotiated contract terms with payers on the Medicare cost written report. Nosotros also are pleased that the bureau recognizes that the COVID-xix pandemic has resulted in not-representative functioning in its hospital quality measurement and value programs, requiring temporary policy adjustments. While CMS' new quality measure on the rate of wellness care personnel COVID-xix vaccination probable needs farther refinement to ensure information technology accurately reflects hospitals' progress in vaccinating their workforce, nosotros will work with CMS, CDC and hospitals to facilitate the reporting of the measure starting on Oct. 1. Lastly, we appreciate that CMS is continuing to review comments on its organ acquisition and Medicare-funded residency slot proposals. We wait forward to working with the agency to develop workable policies. See AHA'southward full statement that was shared with the media here.
Highlights of the inpatient PPS rule follow.
Inpatient PPS Payment Update
The final rule will increase inpatient PPS rates by a net of 2.5% in FY 2022, compared to FY 2021, after accounting for inflation and other adjustments required past police force. Specifically, the update includes an initial market-basket update of ii.vii%, less 0.7 percentage points for productivity required by the Affordable Care Human activity (ACA), and plus 0.5 pct points to partially restore cuts made as a issue of the American Taxpayer Relief Human action (ATRA) of 2012. Table ane below details the factors CMS includes in its approximate.
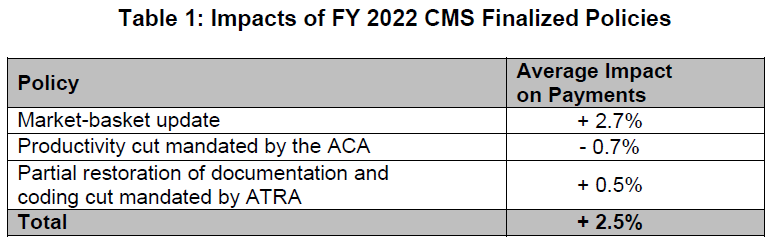
The ACA and ATRA adjustments will exist applied to all hospitals. Additionally, hospitals not submitting quality information will be subject to a one-quarter reduction of the initial market basket and, thus, will receive an update of 1.83%. Hospitals that were not meaningful users of EHRs in FY 2019 will be discipline to a three-quarter reduction of the initial marketplace basket and, thus, volition receive an update of 0.48%. Hospitals that fail to meet both of these requirements will exist subject to a full reduction of the initial market-basket rate and receive an update of -0.20%.
In light of the COVID-19 PHE, CMS finalized that information technology will utilise FY 2019 information in approximating expected FY 2022 inpatient hospital utilization for charge per unit-setting purposes.
Market-based MS-DRG Information Collection and Weight Adding
CMS finalized its repeal of the requirement that hospitals report their median payer-specific negotiated rates for inpatient services, by Medicare Severity-Diagnosis Related Grouping, for Medicare Reward organizations. It also repealed the market-based MS-DRG relative weight methodology CMS had planned to implement in FY 2024; instead, CMS will continue using its existing cost-based methodology.
Disproportionate Share Hospital (DSH) Payment Changes
Under the DSH program, hospitals receive 25% of the Medicare DSH funds they would have received under the former statutory formula (described as "empirically justified" DSH payments). The remaining 75% flows into a separate funding pool for DSH hospitals. This pool is updated as the percentage of uninsured individuals changes and is distributed based on the proportion of total uncompensated care each Medicare DSH hospital provides. For FY 2022, CMS estimates the 75% pool to exist approximately $10.48 billion. Afterward adjusting this pool for the percent of individuals without insurance, CMS estimates the uncompensated intendance corporeality to be approximately $7.nineteen billion, a decrease of roughly $1.1 billion compared to FY 2021.
The agency finalized that it will use a single year of uncompensated care data from Worksheet S-x to determine the distribution of DSH uncompensated intendance payments for FY 2022. Specifically, CMS will employ S-ten data from FY 2018 cost reports, which the agency has recently audited.
Maintenance of the ICD-10-CM and ICD-x-PCS Coding Systems
CMS is adopting an April 1 implementation date for ICD-10-CM and ICD-10-PCS lawmaking updates, in addition to the annual October 1 update, outset with Apr 1, 2022. CMS acknowledges the concerns expressed by the AHA with respect to potential operational problems and with commercial payers and compliance bug. CMS intends to work with stakeholders and identify how the agency tin accost issues that may ascend in this process.
Complication/Comorbidity (CC) and Major Complication/Comorbidity (MCC) Assay
In the proposed rule CMS solicited comments on adopting a change to the severity level designation of the 3,490 "unspecified" diagnosis codes currently designated as either CC or MCC, where at that place are other codes bachelor in that code subcategory that further specify the anatomic site, to a Non-CC for FY 2022. If canonical, the alter would have afflicted the severity level assignment for four.8% of the ICD-ten-CM diagnosis codes. Notwithstanding, for FY 2022, CMS is maintaining the severity level designation of all "unspecified" diagnosis codes on Table 6P.2a. Instead, CMS is finalizing the Unspecified Code Medicare Lawmaking Editor edit which CMS believes provides additional time to brainwash coders on updated coding guidelines and offer assist to providers on proper documentation while not affecting the payment the provider is eligible to receive.
In addition, at the AHA'south recommendation, 58 ICD-ten-CM diagnosis codes will not be included for consideration of irresolute the severity level designation as part of the list of "unspecified" diagnosis codes. The 58 diagnosis codes include malignant neoplasms, occipital fractures, spinal fractures and other internal injuries that cannot be visualized externally.
New Engineering Add-on Payment (NTAP)
The inpatient PPS provides additional payments, known as NTAPs, for cases with relatively high costs involving eligible new medical services or technologies. For FY 2022, in connectedness with CMS' use of the FY 2019 instead of FY 2020 data for rate setting, the agency finalized a ane-year extension of NTAPs for 13 technologies for which the payments would otherwise be discontinued starting time FY 2022.
New COVID-19 Treatments Add together-on Payment (NCTAP)
In response to the pandemic, CMS established the New COVID-xix Treatments Improver Payment (NCTAP) for eligible discharges during the PHE. CMS is extending the NCTAP for eligible COVID-19 products through the end of the fiscal yr in which the PHE ends. Hospitals will be eligible to receive both NCTAP and the traditional NTAP for qualifying patient stays, through the end of the fiscal year in which the PHE ends.
Surface area Wage Index
CMS finalized several policies around the surface area wage index, which adjusts payments to reverberate differences in labor costs across geographic areas. First, the bureau will go on its low-wage-index hospital policy equally established in the FY 2020 concluding dominion. Specifically, for hospitals with a wage index value below the 25th percentile, the agency will keep to increase the infirmary's wage index past half the difference betwixt the otherwise applicable wage index value for that infirmary and the 25th percentile wage index value for all hospitals. As it has done previously, the agency will reduce the FY 2022 standardized amount for all hospitals to make this policy upkeep neutral.
2d, as required past the American Rescue Plan Deed, CMS will permanently reinstate a minimum expanse wage index for hospitals in all-urban states, known equally the "imputed rural flooring." Previously, for FYs 2019 – 2021, hospitals in all-urban states received a wage index without the awarding of an imputed flooring. Per the law, this reinstated policy is non budget neutral and does not require reductions to the standardized amount.
Tertiary, as a result of adopting updates from the Office of Management and Budget's (OMB's) core-based statistical area modifications, CMS last year finalized a policy to cap any decrease in a hospital's last FY 2021 wage alphabetize compared to its last FY 2020 wage index at v%. This was fix to expire at the cease of FY 2021. Withal, CMS is extending this cap through FY 2022 for hospitals that received information technology in FY 2021. Specifically, it will utilize a 5% cap on any decrease in those hospitals' wage alphabetize compared to FY 2021. CMS is applying this policy in a budget-neutral manner.
Finally, CMS is finalizing provisions in the interim concluding dominion it published meantime with the FY 2022 proposed rule, which volition make technical amendments to current regulations related to how certain hospitals tin can be reclassified through the Medicare Geographic Nomenclature Review Board.
Indirect and Direct Medicare Graduate Medical Teaching (GME)
CMS proposed to implement several provisions of the Consolidated Appropriations Human activity, including its requirement for 1,000 new Medicare-funded medical residency positions, the Promoting Rural Infirmary GME Funding Opportunity, which would allow sure rural grooming hospitals to receive a GME cap increment, and the determination of direct GME per-resident amounts and sure full-time equivalent (FTE) resident limits for hospitals that host a minor number of residents for a brusque duration. The agency stated that due to the number and nature of the comments it received on the implementation these programs, it will address these policies in future rulemaking.
Organ Conquering Payment
CMS proposed to codify into Medicare regulations some longstanding Medicare organ acquisition payment policies, as well as some new policies, including clarifying definitions of "transplant hospital," "transplant program" and "organs." In add-on, CMS proposed that transplant hospitals and organ procurement organizations count and report Medicare usable organs to ensure such organs are accurately allocated to Medicare. Lastly, the agency besides proposed several provisions for donor customs hospitals, including reducing its customary charges to its costs.
The agency stated that due to the number and nature of the comments it received on these payment policies, it volition accost these policies in future rulemaking.
Medicare Shared Savings Program (MSSP)
Due to the uncertainty of the COVID-19 pandemic, CMS volition allow accountable care organizations (ACOs) participating in the "Bones" track'southward glide path to forgo automatic advancement and in one case once more "freeze" their participation for performance year (PY) 2022 at their PY 2021 level. CMS first finalized such a policy in last year's physician fee schedule final rule, allowing ACOs to freeze their PY 2020 participation level and avoid automated advocacy in PY 2021. ACOs that froze their participation for PY 2021 at their PY 2020 level will now exist permitted to freeze their participation a second time, thus remaining at their PY 2020 participation level for PY 2022. Whatsoever ACO that elects to remain at its current participation level for PY 2022 will be automatically avant-garde to the BASIC track level in which it would accept participated during PY 2023 if it had avant-garde automatically in PY 2022 (unless the ACO chooses to advance more than apace).
For example, an ACO that participated in BASIC Level A for PY 2020 and did not freeze its participation level would take automatically avant-garde to BASIC Level B in PY 2021. If that ACO elects to remain at Level B for PY 2022, instead of advancing to Level C, it would automatically advance to Level D for PY 2023. Similarly, if an ACO participated in BASIC Level A for PY 2020 and did elect to freeze its participation level, it would have participated in BASIC Level A in PY 2021. If that ACO once more elects to remain at Level A for PY 2022, it would automatically advance to Level D for PY 2023.
Promoting Interoperability Program
CMS finalized proposals to keep the 90-day reporting flow for calendar year (CY) 2023 and to increment the reporting period to 180-days for CY 2024. Consistent with policies for the Merit-based Incentive Payment Organisation (MIPS) Promoting Interoperability category, CMS will maintain the Query of Prescription Drug Monitoring Program measure as optional while increasing available bonus points from v points to 10 points and add together a new, optional Health Information Commutation Bi-Directional Substitution measure as a yes/no attestation beginning in CY 2022. Despite concerns raised by AHA, CMS finalized proposals to require eligible hospitals and critical access hospitals to attest to having completed an almanac assessment of all ix Safety Assurance Factors for EHR Resilience (SAFER) Guides and increase the minimum required score from l points to 60 points (out of 100 points) to be considered a meaningful EHR user.
Infirmary Quality Reporting and Value Programs
CMS finalized a number of significant policy changes to business relationship for the affect of the COVID-19 PHE on its hospital quality reporting and value programs. The agency also adopted five new measures for the inpatient quality reporting (IQR) program, while removing iii current IQR measures.
Mensurate Suppression Policy. In light of the COVID-xix PHE, CMS finalized a measure suppression policy that information technology will use across all of its hospital quality measurement and value programs. Nether the policy, CMS volition "suppress" (i.east., not use) mensurate information it believes have been affected past COVID-xix in calculating hospital performance. The agency'due south goal is to ensure hospitals are non rewarded or penalized for their performance based on not-representative quality data afflicted past the pandemic. The suppression policy will exist applied to several programs, equally described below.
Hospital Value-based Purchasing (HVBP). CMS will suppress nigh of the HVBP program's measures for FY 2022, including the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) measures, Medicare Spending per Casher, and five health care associated infection measures. Every bit a result, CMS believes it cannot calculate off-white scores for hospitals nationally, and all hospitals will receive neutral payment adjustments under the VBP for FY 2022. However, CMS will calculate and report measure out scores publicly where viable and appropriate.
For the FY 2023 HVBP program, CMS will suppress the pneumonia mortality mensurate, and remove the claims-based patient rubber indicator (PSI 90) from the HVBP programme permanently.
Hospital Readmissions Reduction Program (HRRP). For the FY 2023 HRRP, CMS volition suppress the pneumonia readmissions mensurate, and exclude COVID-nineteen diagnosed patients from the remaining v measures.
Infirmary Acquired-Status (HAC) Reduction Program. CMS finalized its proposal to suppress performance data from the third and 4th quarters of 2020 in computing HAC Reduction Program performance for FYs 2022 and 2023. When combined with the waiver of the first two quarters of 2020 information CMS adopted concluding year, hospital HAC scores for FYs 2022 and 2023 will be based on truncated performance periods.
Inpatient Quality Reporting (IQR). CMS finalized its proposal to add together 5 new measures to the IQR program. Virtually notably, CMS adopted new measures reflecting COVID-19 vaccination coverage among health intendance personnel and adoption of practices to reduce maternal morbidity. Both measures must exist reported starting on Oct. ane. CMS besides finalizes the removal of 3 IQR measures. However, based on stakeholder feedback, the agency volition retain two measures information technology had proposed for removal – anticoagulation therapy for atrial fibrillation/flutter electronic clinical quality measure (STK-03) and the death charge per unit among surgical inpatients with serious treatable complications (PSI-04). Beginning in CY 2023, hospitals will be required to report the IQR's eCQMs using certified EHR engineering science consistent with 2015 Edition Cures Update.
Side by side STEPS
The terminal dominion will be published in the Aug. 13 Federal Annals and provisions will generally have effect Oct. 1. Sentry for a more detailed AHA analysis of the last rule in the coming weeks.
If yous have further questions, contact Shannon Wu, AHA senior acquaintance director of policy, at 202-626-2963 or swu@aha.org.

What Is The Latest Version Of The Final Rule For The Ltch Pps In The Fedral Register?,
Source: https://www.aha.org/2021-08-03-aha-summary-hospital-inpatient-pps-final-rule-fiscal-year-2022
Posted by: juarezalloss.blogspot.com
0 Response to "What Is The Latest Version Of The Final Rule For The Ltch Pps In The Fedral Register?"
Post a Comment